Loading...
Antenatal care is the routine health control of presumed healthy pregnant women without symptoms (screening), in order to diagnose diseases or complicating obstetric conditions without symptoms, and to provide information about lifestyle, pregnancy and delivery.
Antenatal care is a key component of a healthy pregnancy. Regular antenatal care helps to identify and treat complications and to promote healthy behaviors. Outcome data suggest that babies born to mothers who do not receive antenatal care are 3 times more likely to be of low birth weight, and 5 times more likely to die, compared with babies born to mothers who receive prenatal care. In addition to medical care, antenatal care includes counseling and education. This monograph provides an overview for the antenatal management of healthy pregnant women with singleton pregnancies.
The guideline has been developed with the following aims: to offer information on best practice for baseline clinical care of all pregnancies and comprehensive information on the antenatal care of the healthy woman with an uncomplicated singleton pregnancy. It provides evidence-based information for use by clinicians and pregnant women to make decisions about appropriate treatment in specific circumstances. Women should be the focus of maternity care, with easy access and continuity of care.
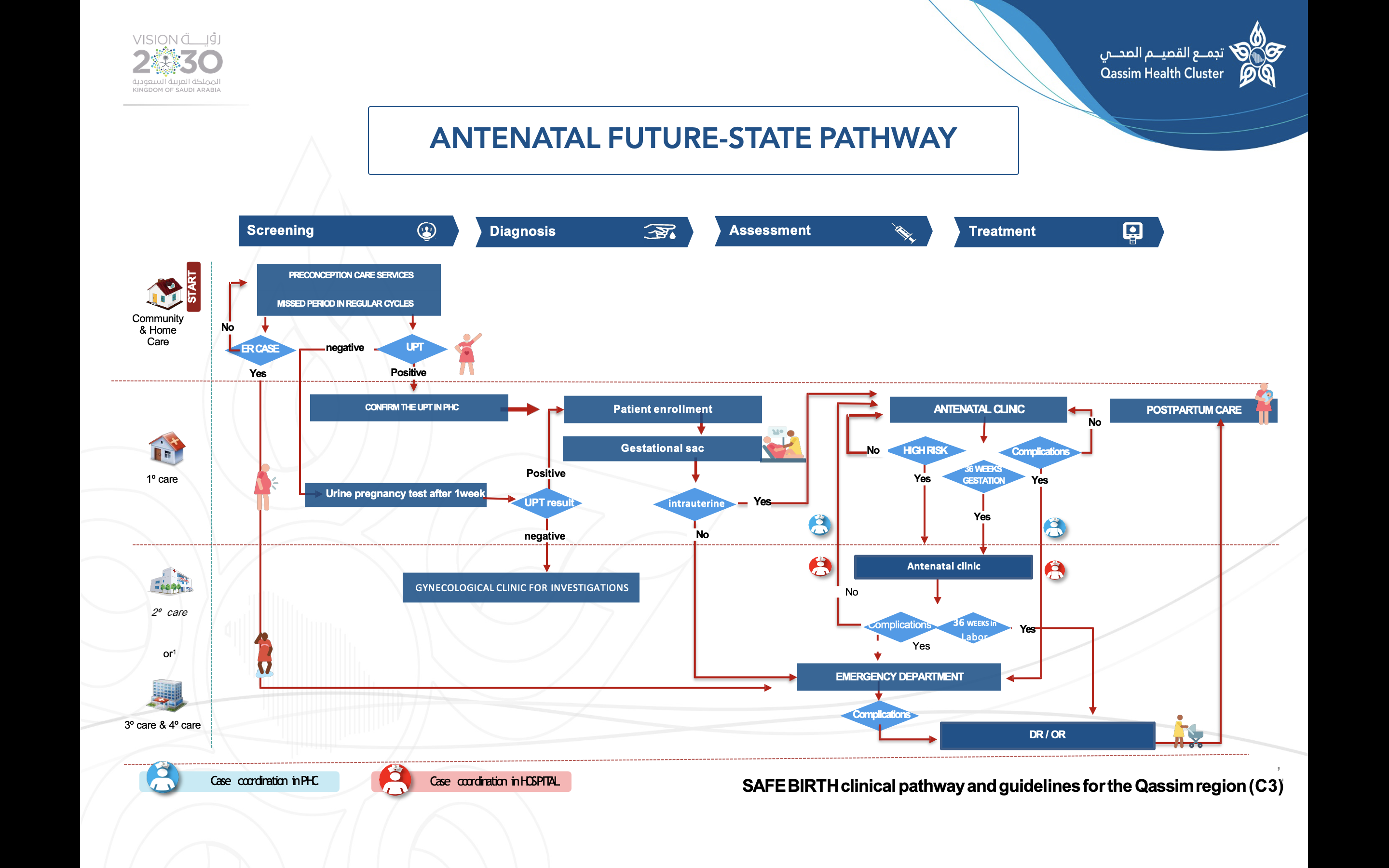
Missed period in regular cycles
if regular cycle, follow the pathway
if irregular cycles, do UPT
if positive – confirm pregnancy diagnostic
if negative – gynecological clinic investigations
Pregnancy diagnostic investigations
Transvaginal/ abdominal ultrasound
B-HCG
Patient enrollment
Client electronic file completed
Vitals, weight, height taking
Registration in health passport & clinic registry
Evaluation by the clinic doctor
Suitable education
Mawid with date + medication
Gestational age
5. Very high risk is patients with symptoms < 6 hours with or without comorbidity
6. Presumptive, Probable and Positive signs of pregnancy:
Registration + history + vital then evaluation by doctor
Clinical examination
Lab investigations
Rubella antibodies
Hepatitis status
VDRL(RPR)
thyroid function test)
Ultrasound
Pharmacy
Appointment
No risk factor12 up to 36 weeks
12 up to 36 weeks
PHC
38 up to 40 weeks
PHC+ ANC on Hospital
Vital signs: Temperature<38°C, SBP≥140 or DBP≥90
12 up to 36 weeks
PHC + emergency transfer to hospital secondary of tertiary
38 up to 40 weeks
PHC + emergency transfer to hospital secondary of tertiary
Vital signs: Maternal HR>120 or <50, temperature≥38.3°C, RR>26 or <12, SPO2<95%, SBP≥140 or DBP≥90, symptomatic or <80/40, FHR>160bpm for >60 seconds; decelerations
12 up to 36 weeks
PHC + emergency transfer to hospital secondary of tertiary
38 up to 40 weeks
PHC + emergency transfer to hospital secondary of tertiary
Vital signs:
*. Maternal HR<40 or >130, SPO2<93%, SBP≥160 or DBP≥110 or <60, FHR<110bpm for >60 seconds, symptomatic or <80/40, FHR>160bpm for >60 seconds; decelerations
*. Immediate lifesaving intervention required, such as: Maternal
Cardiac compromise
Severe respiratory distress
Seizing
Hemorrhaging
Acute mental status change or unresponsive (cannot follow verbal commands)
Signs of placental abruption
Signs of uterine rupture
*. Fetal – prolapsed cord
*. Immediate birth: Fetal parts visible on the perineum, active maternal bearing (down efforts)
12 up to 36 weeks
PHC + emergency transfer to hospital secondary of tertiary
38 up to 40 weeks
PHC + emergency transfer to hospital secondary of tertiary
Non-urgent attention such as
*. >37 weeks’ early labor sings and/ or SROM/ leaking
*. Non-urgent symptoms may include:
common discomforts of pregnancy
vaginal discharge
constipation
ligament pain
nausea
anxiety
12 up to 36 weeks
PHC + emergency transfer to hospital secondary of tertiary
38 up to 40 weeks
PHC + emergency transfer to hospital secondary of tertiary
If the pregnant woman has one or more of the risk factor sin classigying pregnant women with the mother’s health passport
12 up to 36 weeks
PHC + ANC on Hospital
38 up to 40 weeks
PHC + ANC on Hospital
Should not enter through the management pathway in PHC
Should referred immediately to the nearest hospital ER, better by an ambulance
If collapsed, resuscitation measures should be carried out immediately while preparing for immediate transferring to the nearest hospital ER.
Genetic counseling and testing should be offered to couples with a family history of genetic disorders, a previously affected fetus or child, or a history of recurrent miscarriage.
Medical teams and female doctors:
Patients are assigned to doctors according to their clinical records
Patents refusing to see a male doctor will be seen by a female when available of the same caliber
The presence of an appropriately trained female doctor cannot be guaranteed in the antenatal clinics or labor ward all the time
When appropriately trained female doctor is not available and patient refusing-to be seen by a male doctor, patient is informed that she takes her own responsibility.
The initial visit should occur during the first trimester to identify women who may need additional care and plan pattern of care for the pregnancy
The estimated date of delivery (EDD) should be calculated by accurate determination of the last menstrual period (LMP)
Early ultrasonography is more accurate than LMP at determining gestational age, and that it should be used routinely to determine EDD and reduce the need for labor induction. If pt. More than 8 weeks, cheek for viability by USS, then request official us for dating and nt between 11-13 weeks
Information about physiologic changes that occur during pregnancy and preparation for the birthing process are key themes around which to discuss care issues and choices such as breastfeeding
VTE risk assessment. ▪ if high risk for PTL — screen for bacterial vaginosis
Pap smear will be offered preferably in first trimester if it was not done in last 3 yrs
Folic acid 1mg to be started as soon as pregnancy diagnosed
Lab investigation: CBC, blood group, RH type, RBS, serology for HIV, hepatitis C & B, complete urine analysis.
Medication
Folic Acid 1mg, OD during the first 23 months of pregnancy
Fe fumarate (200mg) or Sulphate 60mg
O.D. if Hb is 10.5gm/dL
B.D if Hb is <10.5gm/dL
Prenatal Education
Information about physiologic changes that occur during pregnancy and preparation for the birthing process are key themes around which to discuss care issues and choices such as breastfeeding
Patients following in secondary and tertiary center will be seen weekly from 36 weeks till 40 weeks
At 41 weeks’ patient will be counseled for induction of labor (IOL) if no onset of spontaneous labor
In those anemic: Diet, compliance, the iron chelating agents should be revised
The patient should be asked about fetal movements and this should be recorded in the file
Any complaint should be documented
BP should be checked by the nurse while the patient is "sitting" (which is easier and quicker than the left lateral position) if BP is >140/90 it should be rechecked by the doctor after 30 minutes
The patient will be weighted regularly and her weight gain" should be observed
Routine urine analysis should be routinely done for every patient upon arrival to the OPD
Symphysis fundal (S.F.) height should be checked routinely for gestations between 26 to 36 weeks
The S.F.H. should be with in 3cm (+ or-) of the gestational age in weeks. ▪ presentation of the fetus should be documented ▪ an ultrasound scan should be done at18-22 weeks for anomaly, and arrange visit to review report
At 28 weeks, repeat CBC, review results of GDM screening, repeat ICT if she is RH negative & consider anti-D if needed
CBC
Frequency
At the booking visit
26 weeks and 34 weeks’ gestation visits
Indication
Blood group & type
Anemia
According to the case, other parameters
Instructions
Fasting not required
Venous blood
Aseptic technique
Serum ferritin
Frequency
At the booking visit
26 weeks’ gestation
If indicated (any visit)
Indication
Type of anemia (if present)
Instructions
Fasting not required
Venous blood
Aseptic technique
HA1C
Frequency
At the booking visit (if indicated)
Indication
Evaluation of already established DM
Instructions
Fasting not required
Venous blood
Aseptic technique
OGTT 75 GM
Frequency
At 26-28 weeks’ gestation those at risk of GDM
Indication
For GDM diagnosis
Instructions
Fasting for 8-14 hours
Venous blood before taking PO glucose solution
1hour post prandial
2hours post prandial
Urine analysis
Frequency
Every visit
Indication
To investigate UTI, PET, glycosuria, hematuria and aceton
Instructions
1st catch midstream urine
Indirect coomb’s test
Frequency
Once (booking visit)
Indication
If RH-VE (to detect antibodies)
Instructions
Venous blood
Mother Health Passport, Saudi Arabia, 2020
Maternal Fetal Triage Index (MFTI), United States, 2016
Model of Care (Safe birth) Antenatal Care Services, King Saud Medical City, Saudi Arabia, June 17, 2018
Segment 0: very low risk – referred to PHC
Segment 1: low risk – PHC + Antenatal on Hospital
Segment 3: very high risk – PHC +Emergency transfer to hospital secondary or tertiary
*. Non eligible case – women requiring additional care, any woman with one or more risk factor – referred to the hospital
*. Eligible case – uncomplicated pregnancy is a singleton gestation without maternal or fetal risk factors
{kind=link}