Loading...
The Urgent Care Clinics project is an initiative to establish walk-in clinics that provide immediate medical attention for minor illnesses and injuries that are urgent but not severe enough to necessitate a visit to a hospital emergency room. These clinics are designed to be easily accessible, offering a vital healthcare service that bridges the gap between traditional doctor's appointments and emergency room care. The project aims to enhance community health by delivering timely and efficient care, reducing the strain on hospital emergency departments, and ensuring patients receive the right level of care for their acute medical needs. This initiative is crucial for stabilizing patients quickly and effectively, thereby improving overall patient outcomes and satisfaction.
Special definitions related to UCC:
Urgent Care Clinic is a walk-in clinic focused on the delivery of medical care for minor illnesses and injuries in an Ambulatory Medical Facility outside of a traditional Hospital-based or freestanding emergency department.
Urgent Medical Care is the care provided for the patients with acute illnesses or injuries which require immediate medical attention to provide acute interventions for patient stabilization.
Urgent Medical Case is a medical case with sufficient severity such that the absence of immediate medical attention could place the individual’s health at risk.
· UCC will provide a continuous journey of health care for the patient through appropriate assessment ,provision of definitive care Undertaking the maximum number of low acuity patient .
· Patients greater flexibility for accessing healthcare services that require minimal intervention..
· Provide cost saving medical care vs the E.D.
· Improve Patient Experience and satisfaction for low acuity acute illness
· Screening opportunities to improve population health
UCCs aim to reduce the pressure on Ed departments (reducing the percentage of CTAS4-5 cases in ED hospitals )through 23 urgent care clinics in Qassim cluster.
Urgent Care Clinics (UCCs) emerged as a response to the growing need for accessible, immediate medical care for conditions that are urgent but not severe enough to require emergency department resources. The history of urgent care dates back to the 1970s in the United States, where the first clinics were established to address the inefficiencies and high costs associated with hospital emergency rooms for treating minor ailments.
The concept quickly gained popularity due to its practicality and patient-centered approach, offering extended hours and accepting walk-ins without prior appointments, which significantly improved access to care. Over the decades, the urgent care model has evolved to include a broad range of services such as imaging and laboratory tests, which traditionally were only available in hospital settings.
Internationally, the model has been adapted to fit different health systems and patient needs, always focusing on bridging the gap between primary care and emergency services. This has contributed to reducing wait times in emergency rooms and providing more focused care, improving both cost efficiency and patient satisfaction in healthcare systems around the world.
In the Qassim Health Cluster, the Urgent Care Clinics (UCCs) initiative has been strategically developed to enhance the region's healthcare delivery system by providing timely and efficient care for non-critical urgent cases. This initiative is part of a broader effort to manage the patient load effectively, reduce the burden on hospital emergency departments, and ensure that acute but non-life-threatening conditions are addressed promptly and appropriately.
The UCCs in the Qassim Health Cluster are designed to integrate into the existing healthcare infrastructure, making use of the multidisciplinary medical teams and facilities already in place. These clinics not only serve to offload the emergency departments by treating cases categorized as Canadian Triage and Acuity Scale (CTAS) levels 4 and 5 but also aim to improve the overall patient care journey by offering services closer to the community.
This initiative reflects an understanding of the local healthcare needs and the challenges faced by the emergency services in the region. By optimizing the use of resources and enhancing care pathways, the Qassim Health Cluster's UCCs are pivotal in improving healthcare accessibility and efficiency within the community, thus aligning with national healthcare goals and strategies.
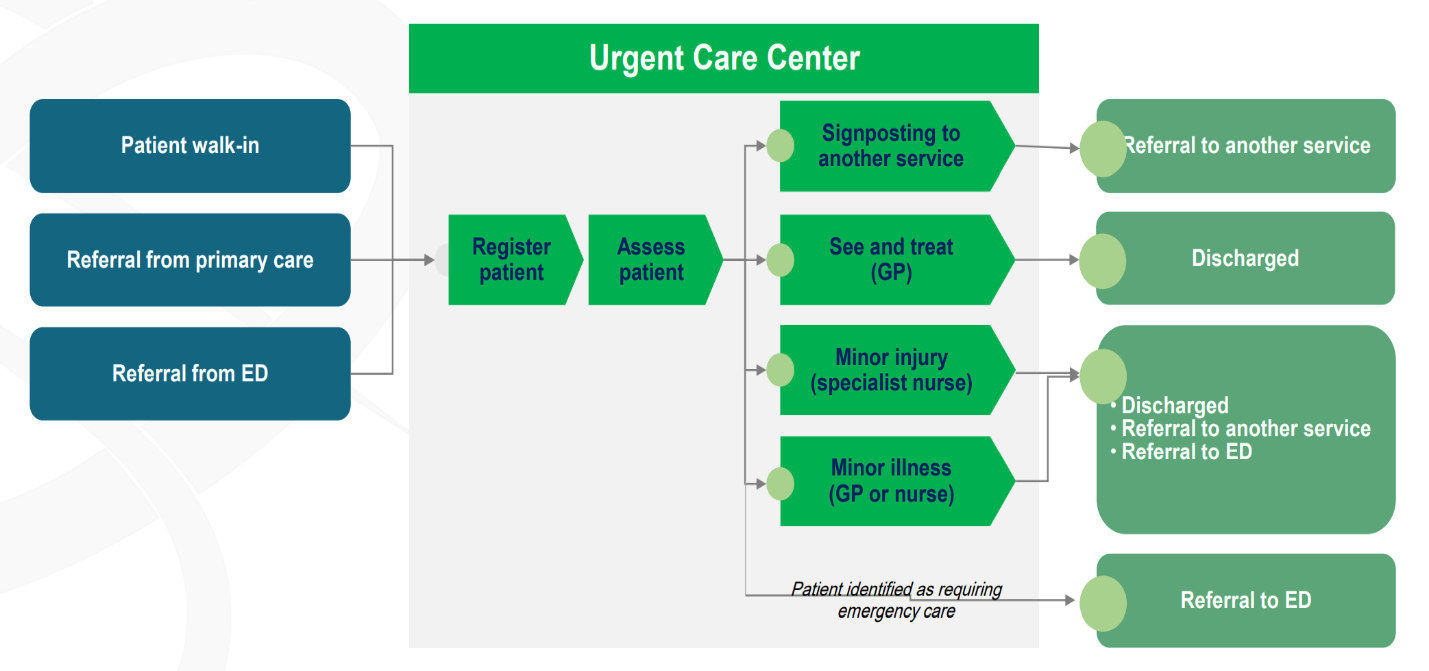
Upon patient arrival at the UCC, all patients, whether walk-in or referred from other healthcare facilities, are promptly registered by the reception staff then transfer to triage station.
Triage is a sorting process utilizing critical thinking and a standardized set of guidelines in which an experienced healthcare practitioner assesses patients quickly upon arrival for the following purpose:
1. Assess and determine severity of presenting problems
2. Process patients into triage category and assigning to an appropriate location.
3. Determine access to appropriate treatment
4. Effectively and efficiently assign appropriate healthcare practitioners for a specific case Process patients into triage category and assigning to an appropriate location.
The Canadian Triage and Acuity Scale (CTAS) is a tool used both nationally and internationally to allow healthcare centers and their staff to prioritize patient care requirements. CTAS has five acuity levels that extend from life threatening conditions (CTAS 1) that require immediate attention to conditions that are non-urgent (CTAS 5) or that may be part of a chronic problem.
A physician or a qualified nurse at the reception area conducts an initial assessment using the CTAS to determine the urgency of the patient's condition. The CTAS categorizes patients into five levels based on the severity of their presenting problem, ranging from life-threatening (Level 1) to non-urgent (Level 5).
Chief Complaint: The nurse evaluates the onset, course, duration, and intensity of the patient's symptoms, including pain scale assessment if applicable.
Physical Assessment: A rapid, concise physical assessment is conducted, focusing on identifying urgent medical needs and priorities for care.
Vital Signs: The patient's vital signs, including heart rate, blood pressure, respiratory rate, and temperature, are measured to assess their physiological status
Patients are continuously monitored for any changes in their condition while waiting for further evaluation or treatment.
Reassessment may be conducted periodically, especially for patients categorized as Level 3 or below, to ensure timely identification of any deterioration or change in acuity.
Each CTAS category is associated with a corresponding timeframe for patients to be seen by a physician. Here's how CTAS categorizes patients in the UCC along with the time to physician:
· Description: Patients with life-threatening conditions requiring immediate intervention to stabilize vital functions.
· Examples: Cardiac arrest, severe trauma with unstable vital signs, respiratory failure requiring immediate intubation.
· Time to Physician: Immediate
· Description: Patients with potentially life-threatening conditions requiring rapid assessment and intervention.
· Examples: Chest pain suggestive of acute coronary syndrome, acute respiratory distress without imminent respiratory failure, severe allergic reactions.
· Time to Physician: Within 15 minutes
· Description: Patients with urgent medical conditions requiring timely assessment and treatment.
· Examples: Suspected fractures or dislocations, moderate asthma exacerbations, acute abdominal pain without signs of peritonitis.
· Time to Physician: Within 30 minutes
· Description: Patients with non-life-threatening conditions requiring medical attention, but not urgently.
· Examples: Minor injuries (e.g., lacerations requiring suturing), urinary tract infections without systemic symptoms, mild exacerbations of chronic conditions.
· Time to Physician: Within 2 hours
· Description: Patients with non-urgent conditions requiring medical assessment and intervention.
· Examples: Minor cuts and bruises, upper respiratory tract infections without complications, routine medication refills.
· Time to Physician: Within 2 hours
By adhering to these CTAS categories and associated timeframes, the UCC ensures that patients receive timely and appropriate medical care based on the urgency of their conditions. This approach helps prioritize patient needs, optimize resource allocation, and improve overall patient outcomes within the clinic.
1. Quality Assurance and Continuous Improvement:
· Conduct regular audits and quality measures to assess management plan effectiveness.
· Use feedback from patients, staff, and stakeholders to improve care protocols.
2. Documentation and Communication:
· Ensure all treatments and patient responses are accurately documented in electronic medical records.
· Maintain clear communication among healthcare team members for coordinated care and seamless transitions.
3. Emergency Preparedness:
· Maintain readiness for unexpected emergencies with regular staff training and protocols for rapid response.
· Keep emergency equipment and medications readily available.
4. Patient Advocacy and Empowerment:
· Encourage patient participation in care decisions, emphasizing informed consent and shared decision-making.
5. The Referral Policy and Procedure to ER:
· Adhere to established policies for referrals within and outside the Qassim Region.
· Ensure all transfers, especially unstable cases, are conducted efficiently with qualified staff.
• Upon arrival, patients are promptly assessed using the Canadian Triage and Acuity Scale (CTAS) by a qualified nurse.
• Chief complaint, physical assessment, and vital signs are evaluated to determine the urgency of the patient's condition.
• Patients categorized as Levels 4 and 5 indicate less urgent or non-urgent conditions that can be managed within the UCC, while higher acuity levels (CTAS 1-3) may require immediate referral to the hospital ED.
• Patients receive timely treatment based on their triage category and presenting symptoms.
• Treatment modalities may include:
• First aid measures.
• Diagnostic services such as laboratory tests and radiological imaging.
• Pharmacological interventions for pain management or symptom relief.
• Therapeutic procedures including suturing, wound dressing, and splinting.
• Patients are continuously monitored for any changes in their condition during treatment.
• If necessary, patients may be referred to specialty services within the UCC or to the hospital ED for further evaluation.
• Consultation with specialists such as radiologists, pharmacists, and laboratory physicians is available as needed to optimize patient care.
• Patients are discharged from the UCC with a comprehensive plan of care.
• Discharge instructions include guidance on self-care, medication management, and signs of worsening symptoms requiring immediate medical attention.
• All interventions, treatments, and patient responses are accurately documented in the electronic medical record.
• Clear communication is maintained among the healthcare team members to ensure coordinated care and seamless transitions for the patient.
• Patients and their caregivers receive education regarding their condition, treatment options, and steps to promote recovery.
• Emphasis is placed on medication adherence, lifestyle modifications, and recognizing warning signs necessitating further medical attention.
• Regular audits and quality assurance measures are conducted to assess the effectiveness of the management plan.
• Feedback from patients, staff, and stakeholders is utilized to identify areas for improvement and implement necessary changes in patient care protocols.
• The UCC maintains readiness to manage unexpected emergencies through regular staff training, drills, and protocols for rapid response.
• Emergency equipment and medications are readily available to ensure timely intervention in critical situations.
• Patients are empowered to participate in decision-making regarding their care, with emphasis on informed consent and shared decision-making principles.
• Patient with minor injury or illness is directed to the Physician or Nurse Specialist. Thereafter, according to the patient’s condition, whether the patient is discharged, referred to a specific specialty or another service or referred to the Emergency Department (ED)Patients who categorized as Level 3 and below on arrival are re-triaged by the UCC Physician.
• Patients identified as requiring emergency care after the re-assessment, they are timely referred to the Emergency Department according to the urgency of the case:
• Transfer of all cases post resuscitation shall be by UCC ambulance and with accompanying qualified staff certified with advanced lifesaving trainings i.e. ACLS/PALS/ATLS/NRP
• Referrals from ER that are according to the scope of UCC Level 4 and 5 shall be accepted and managed in UCC.
• All referrals shall adhere to the established general policy for referrals inside and outside Qassim Region.
• Referrals of beneficiaries of Urgent Care Clinic within the Qassim Region Health Facilities shall adhere to this policy of Urgent Care Clinic of Emergency/Lifesaving Cases.
• Emergency Referral (Unstable) – Immediate transfer by ambulance through the emergency operation center in Qassim Health Cluster to notify the designated ER Department accompanied with a Qualified healthcare practitioner (physician and nurse) trained on ACLS/PALS (or BLS).
All referrals are based on the opinion of the Treating Medical Team with the Treating Physician’s name and contact information written and stamped on the Referral Form.
• All responses to referrals must be clear medical response and no transfers to other Hospitals shall be done without the response.
• For all referrals, patient ID (National ID/IQAMA) and patient information form are attached, ensuring that the patient data written is correct.
• The reason for transfer must be clearly stated.
• The patient’s report must include the medical history, treatment given, latest vital signs, and results of investigations i.e. Laboratory / Radiology if any.
• All referrals are made through the Electronic Referral System.
• Notify the Qassim Health Cluster operation by Contact the hotline number (+966 16 323 6168).
• Transferred Red Case patient must be accompanied with Qualified health practitioner team ACLS/PALS (or BLS) nurse and physician.
• The Medical Coordination in the UCC and ER must be provided with the daily list of physicians on duty i.e. On call Physician Schedule and their On call contact number.
• All observations are monitored daily through a Status Report that is submitted monthly to the Coordination Department for Medical Referrals for review and work to non-recurrence.
• The referring Facility (UCC in Primary Health Center) is responsible for follow-up on the patient’s condition until he is received.
• Once the referral case received by emergency unit in the hospital, the UCC staff will be back to UCC clinic.
• The arrival of the patient is confirmed through the Referral System by the receiving hospital once the patient arrives.
- Pulse oximetry.
- 12 lead ECG.
- Cardiac monitoring.
- Point of Care Testing (POCT)
- CBC
- Glucometer
- Urine dipstick
- Radiological service:
- x-ray
- Ultrasound
- First aid measures with application of the therapeutic protocol for every case.
- Provision of Basic and Advanced Cardiac Life Support.
- Defibrillation
- Fluid replacement and resuscitation.
- Pharmacological drugs.
- Oxygen supply and Nebulizer therapy.
- Pain management, Patient Controlled Analgesia.
- Suturing of cut wounds.
- Dressing of wounds and burns.
- First aid management of sprains and fractures.
- Control of bleeding

Urgent Care Clinics will operate according to either of the following schedules respectively:
24 hours a day, 7 days a week
6 hours a day, 7 days a week
16 hours a day, 5 days a week
Basic Life support Courses for all Medical Staff
Triage Course for nurses and Phscians
Advanced Cardiovascular Life Support (ACLS) For Physcians
Advanced Pediatric Life Support (PALS) for Physcians
Basic Airway management course for Physcians
Common Urgent Cases Management (Medical, Surgical, pediatric, Ob/Gyn) for physcians
Venous access Skills, IV Fluids for nurses
Pre-Hospital Trauma Life Support Course
ECG reading skills for physcians
Common Pediatric Emergencies for physcians
Advanced Trauma Care For Nurses (ATCN) Course for nurses
Training course on how to use the I-STAT device
Advanced Life Support (ATLS) for physcians
UCC 01 مركز صحي الإسكان ببريدة
UCC 02 مركز صحي الشقة ببريدة
UCC 03 مركز صحي السادة ببريدة
UCC 04 مركز صحي الضاحي ببريدة
UCC 05 الاشرفيه في عنيزة
UCC 06 مركزالروضة بالرس
UCC 07 مركز صحي الوسطى بالبدائع
UCC 08 مركز صحي الزهرة في البكيرية
UCC 09 الصفراء في المذنب
UCC 10 خصيبة في الاسياح
UCC 11 ضليع رشيد في ابانات
UCC 12 مركز صحي الفويلق في البكيرية
UCC 13 عيون الجواء
UCC 14 مركز شري في عيون الجواء
UCC 15 مركز صحي الشماسية في الشماسية
UCC 16 الملك خالد في عنيزة
UCC 17 العمار في المذنب
UCC 18 الدليمية في رياض الخبراء
UCC 19 مركز صحي دخنة بالرس
UCC 20 مركز صحي الفوارة بالنبهانية
UCC 21 العاقر في ضرية (ابانات)
UCC 22 مركز صحي عطى في النبهانية
UCC 23 مركز صحي شرق الفايزية ببريدة
SOON (Under preparing ,when it be ready will upload it to an electronic link in this place)

MANUAL FOR EXTENDED WORKING HOURS SERVICES
Urgent Care Center Standard Manual From Health clusterhttps://www.mycme.com/pages/featured-courseshttps://www.mycme.com/pages/featured-courses
1. Urgent Care Pathway: MOH Guide to Excellence in Primary Health Care Centers; Saudi Arabia
2. Follow-up of Patients in Urgent Room Policy and Procedure (ED-IPP-003EA (1)); MOH Urgent Services; June 2017
3. Patient Triage and Priority Policy and Procedures (ED-APP-002-EA): MOH PHC Emergency Services; June 2017
4. Fast Tract Policy and Procedure (KSH/MS/ED-016): King Saud Hospital – Unaizah: Revised 2022
5. Evidenced Based Triage Process (KSH/MS/ED-001): King Saud Hospital – Unaizah: Revised 2022
6. Urgent Care Clinic (UCC) In C3, October 2020
7. Urgent Care Center Standard Manual, Health Holding Company
learninghub.lean. (2023). Retrieved from http://learninghub.lean.sa/
{kind=link}