Loading...
One of the main measures adopted by the Ministry of Health is the model of care. It was introduced as part of the new vision of our country (2030) in 2017. The model represents a method for restructuring health care through interactions between health systems and communities . It focuses on the patient's journey through health system and help to provide an organized, coordinated, and patient centered healthcare services. The outcomes of this model will be reflected on cost reduction, decrease in morbidity and mortality from chronic diseases as well as increase the satisfaction of patients and their caregiver.
We in the chronic care team are working together to improve chronic diseases care in the region that integrate the available resources with the best practices worldwide. We will also engage the healthcare workers at different healthcare levels to activate the role of multidisciplinary team in the management of chronic diseases.

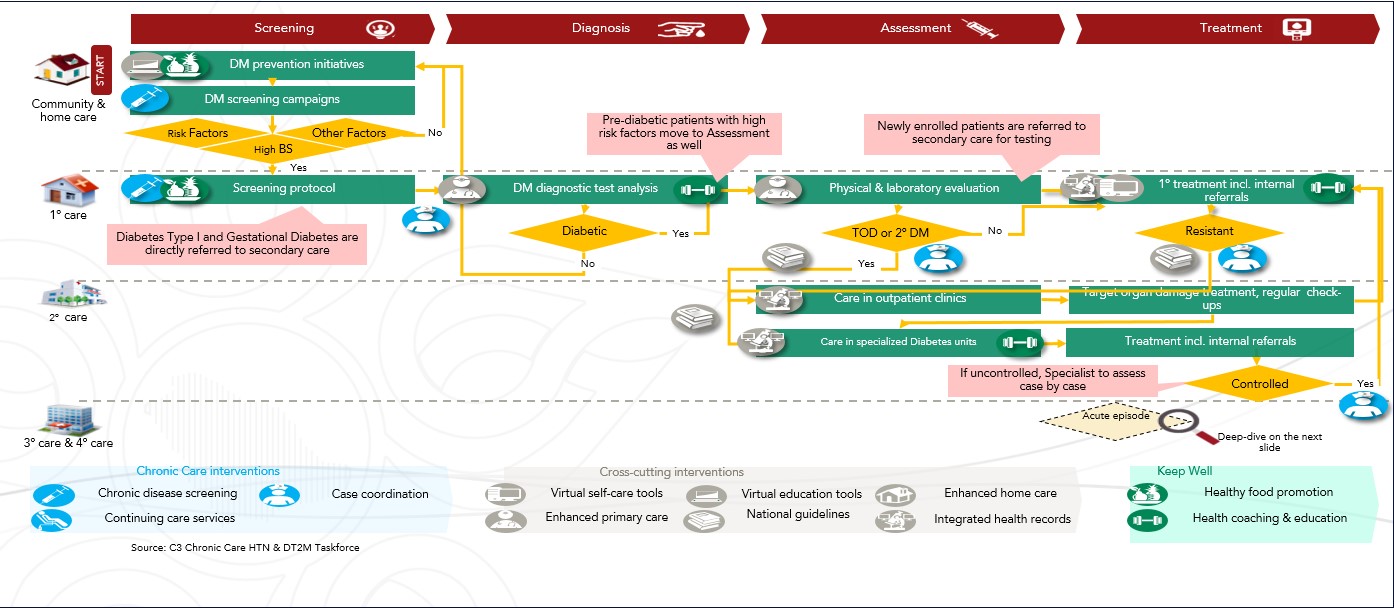
DM Pathway undergo Standers of Care in Diabetes - 2023


Screening for Diabetes Complications:
1.Chronic Kidney Disease:
At least once a year, assess urinary albumin (e.g., spot urinary albumin-to-creatinine ratio) and estimated glomerular filtration rate (eGFR) in patients with type 1 diabetes with duration of ≥5 years and in all patients with type 2 diabetes regardless of treatment.
Patients with urinary albumin >30 mg/g creatinine and/or an eGFR <60 mL/min/1.73 m2 should be monitored twice annually to guide therapy.
2. Diabetic Retinopathy:
Adults with type 1 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist within 5 years after the onset of diabetes
Patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist at the time of the diabetes diagnosis If there is no evidence of retinopathy for one or more annual eye exams and glycemia is well controlled, then screening every 1-2 years may be considered. If any level of diabetic retinopathy is present, subsequent dilated retinal examinations should be repeated at least annually by an ophthalmologist or optometrist.
If retinopathy is progressing or sight-threatening, then examinations will be required more frequently Eye examinations should occur before pregnancy or in the first trimester in patients with preexisting type 1 or type 2 diabetes, and then patients should be monitored every trimester and for 1 year postpartum as indicated by the degree of retinopathy.
3. Neuropathy Screening:
All patients should be assessed for diabetic peripheral neuropathy starting at diagnosis of type 2 diabetes and 5 years after the diagnosis of type 1 diabetes and at least annually thereafter Neuropathy screening: Assessment for distal symmetric polyneuropathy should include a careful history and assessment of either temperature or pinprick sensation (small fiber function) and vibration sensation using a 128-Hz tuning fork (for large-fiber function).
All patients should have annual 10-g monofilament testing to identify feet at risk for ulceration and amputation Symptoms and signs of autonomic neuropathy should be assessed in patients with microvascular complications
4. Foot Care Screening: Perform a comprehensive foot evaluation at least annually to identify risk factors for ulcers and amputations Foot Care Screening: Patients with evidence of sensory loss or prior ulceration or amputation should have their feet inspected at every visit
Refer patient to 2nd or 3rd care if:
Referral back of Diabetic patients from 2ry-3ry Care to PHCs (after the patient is controlled or end the Requested Service) through Case Coordinators should accompanied with Discharge Summary and plan of care (If unified EHR is not available).
Criteria for screening for diabetes or prediabetes in asymptomatic adults
1.Testing should be considered in adults with overweight or obesity (BMI 25 kg/m2 or =23 kg/m2 in Asian Americans) who have one or more of the following risk factors:
• First-degree relative with diabetes
• High-risk race/ethnicity (e.g., African American, Latino, Native American, Asian American, Pacific Islander)
• History of CVD
• Hypertension (140/90 mmHg or on therapy for hypertension)
• HDL cholesterol level <35 mg/dL (0.90 mmol/L) and/or a triglyceride level >250 mg/dL (2.82 mmol/L)
• Women with polycystic ovary syndrome
• Physical inactivity
• Other clinical conditions associated with insulin resistance (e.g., severe obesity, acanthosis nigricans)
2. Patients with prediabetes (A1C ==5.7% [39 mmol/mol], IGT, or IFG) should be tested yearly. 3. Women who were diagnosed with GDM should have lifelong testing at least every 3 years. 4. For all other patients, testing should begin at age 35 years.
5. If results are normal, testing should be repeated at a minimum of 3-year intervals, with consideration of more frequent testing depending on initial results and risk status.
6. People with HIV
CVD, cardiovascular disease; GDM, gestational diabetes mellitus; IFG, impaired fasting glu- cose; IGT, impaired glucose tolerance.
Screening for and diagnosis of GDM
One-step strategy
Perform a 75-g OGTT, with plasma glucose measurement when patient is fasting and at 1 and 2 h, at 24-28 weeks of gestation in women not previously diagnosed with diabetes.
The OGTT should be performed in the morning after an overnight fast of at least 8 h.
The diagnosis of GDM is made when any of the following plasma glucose values are met or exceeded:
• Fasting: 92 mg/dL (5.1 mmol/L)
1 h: 180 mg/dL (10.0 mmol/L)
2 h: 153 mg/dL (8.5 mmol/L)
Two-step strategy
Step 1: Perform a 50-g GLT (nonfasting), with plasma glucose measurement at 1 h, at 24-28 weeks of gestation in women not previously diagnosed with diabetes.
If the plasma glucose level measured 1 h after the load is 130, 135, or 140 mg/dL (7.2, 7.5, or 7.8 mmol/L, respectively), proceed to a 100-g OGTT.
Step 2: The 100-g OGTT should be performed when the patient is fasting.
The diagnosis of GDM is made when at least two* of the following four plasma glucose levels (measured fasting and at 1, 2, and 3 h during OGTT) are met or exceeded (Carpenter-Coustan criteria [244]):
Fasting: 95 mg/dL (5.3 mmol/L)
1 h: 180 mg/dL (10.0 mmol/L)
2 h: 155 mg/dL (8.6 mmol/L)
3 h: 140 mg/dL (7.8 mmol/L)
GLT, glucose load test; OGTT, oral glucose tolerance and Gynecologists notes that one elevated value GDM, gestational diabetes mellitus; test. *American College of Obstetricians can be used for diagnosis (240).
# May also need to be checked after initiation or dose changes of medications that affect these laboratory values (i.e., diabetes, blood pressure, cholesterol, or thyroid medications).
* May be needed more frequently in patients with known CKD or with changes in medications that affect kidney function and serum potassium.
PHC Referral Guidelines:
Refer patient to 2nd or 3rd care if:
Refer patient to acute care centers if either:
Criteria for Referral to Tertiary DM Center:
Case Management Guidelines:
{kind=link}