Loading...
In the Kingdom of Saudi Arabia (KSA), obesity (defined as body mass index (BMI) of ≥30 kg/m2) and overweight (defined as BMI of 25-29.9 kg/m2) represent an alarming threat for population health based on their high prevalence.
Both genders are affected, with some differences existing, where obesity is more prevalent among females, while overweight is higher among males.
The high prevalence is a real concern; especially since obesity and overweight are well known risk factors for several life-threatening conditions including type 2 diabetes, coronary artery disease, hypertension, and certain cancers, in addition to impaired quality of life.
Obesity and its comorbidities are multifactorial (including genetic, environmental, psychological, social, and cultural factors), requiring multiple approaches to population management in various settings with input from a range of stakeholders.
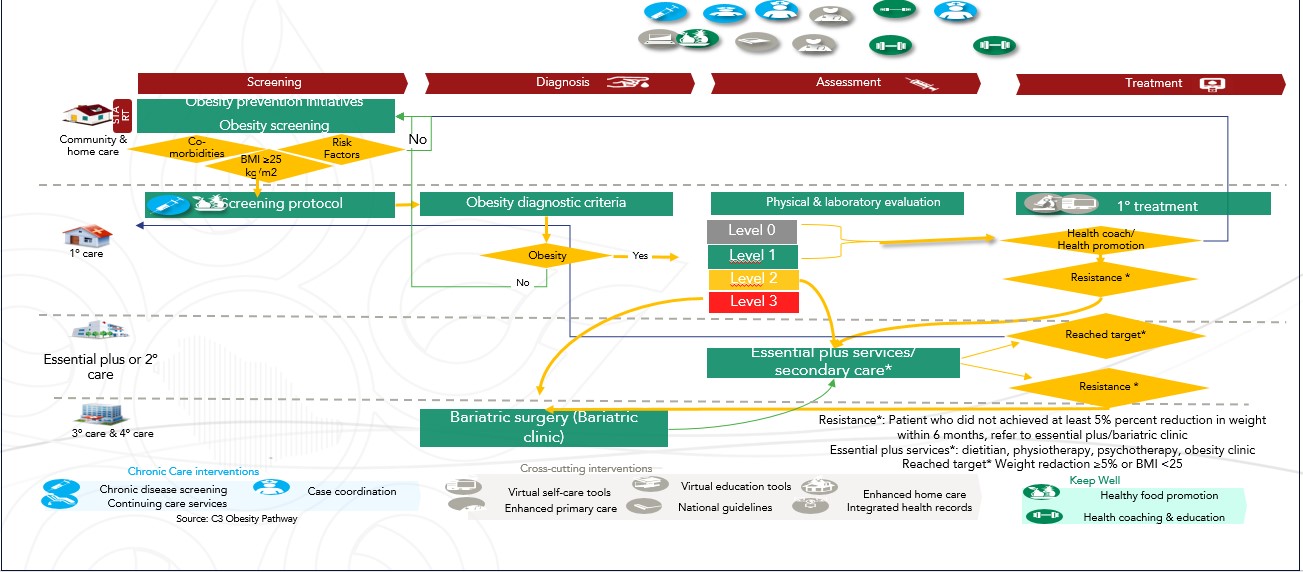
To promote healthy lifestyle in the community and decreasing the number of overweight and obese patients in the whole region of Al Qassim by following these objectives:
1. Patients or population are categorized depending on their BMI into levels.
Patient Segmentation:( Target Population)
2. With the following segmentation:
Level 0
Level 1
Level 2
Level 3
1) subjective assessments
By :
A. History taking and assessing the readiness of the patient
B.focus on getting the patient past history of chronic diseases and any previous attempts for weight loss interventions
C.the patient family history for obesity
D.history of using any medications
E.Surgical history
F.psychological and social history
2)Objective assessment
By:
Clinical examination and labs investigation
Consider bariatric surgery:
{kind=link}