Loading...
Asthma is a common heterogeneous inflammatory chronic disorder of the airways. it is one of the most common chronic diseases in Saudi Arabia, with increasing prevalence. It has significant impact on patients, their families, and the community as a whole in terms of lost work and school days, poor quality of life, frequent emergency department (ED) visits, hospitalizations, and deaths.
The overall prevalence of asthma in children from Saudi Arabia has been reported to range from 8% to 25%, based on studies conducted over the past three decade. This increasing in prevalence of asthma is considered one of the main challenges facing our health systems and society as a whole.
Expiratory airflow limitation is defined as an FEV1/FVC less than the lower limit of normal for age.
In adults and adolescents , an increase in FEV1 ≥200mL and ≥ 12% from baseline 10 to 15 minutes after bronchodilator is a positive bronchodilator response.
In adults and adolescents, asthma control is based on assessing asthma symptoms, use of reliever medications, and impact on daily activities.
There are several methods of assessing symptoms control, including:
The ACT is a commonly used tool to assess asthma control. The score of ACT is the sum of the five questions where each is scored from 1 (worst) to 5 (best), leading to a maximum best score of 25. The level of asthma control is categorized into:

The ACT is a commonly used tool to assess asthma control. The score of ACT is the sum of the five questions where each is scored from 1 (worst) to 5 (best), leading to a maximum best score of 25. The level of asthma control is categorized into:
· Controlled: An ACT score of ≥20
· Partially controlled: An ACT score of 16-19
· Uncontrolled: An ACT score of <16

|
The pediatric respiratory assessment measure (PRAM) score |
||||
|
Sign |
0 |
1 |
2 |
3 |
|
Suprasternal retraction |
Absent |
|
Present |
|
|
Scalene muscle contraction |
Absent |
|
Present |
|
|
Air entry |
Normal |
Decreased at bases |
Widespread decreased |
Absent/ minimal |
|
Wheezing |
Absent |
Expiratory only |
Inspiratory and expiratory |
Audible without stethoscope/ silent chest with minimal air entry |
|
O2 saturation |
≥95% |
92-94% |
<92% |
|
Total score of 1-3: low risk and manage in PHC
Total score of 4-7: moderate risk, refer to hospital ER
Total score of 8-12: high risk, refer to hospital ER
|
Level |
Characteristics |
|
Moderate asthma attacks |
· Increasing symptoms · PERF>50-75% best or predicted · No features of acute severe asthma |
|
Acute severe asthma |
· Any one of: o PEF 30-50% best or predicted o Respiratory rate ≥ 25/min o Heart rate3 120/min · Inability to complete sentences in one breath |
|
Life threatening asthma |
· Any one of the followings in a patient with severe asthma: o SpO2 <92% (PaO2, <60 mmHg) on high flow FIO2 o PEF <30% best or predicted o Bradycardia o Dysrhythmia o Cyanosis o Hypotension o Normal or high PaCO2 o Exhaustion o Confusion o Silent chest o Coma · Weak respiratory effort |
|
Near-fatal asthma |
· Raised PaCO2 and/or requiring mechanical ventilation |
|
Brittle asthma |
· Type 1: Wide PEF variability (>40% diurnal variation for >50% of the time over a period >3-6 months) despite intense therapy · Type 2: Sudden severe attacks on a background of apparently well-controlled asthma |
|
PEF = peak expiratory flow |
|
|
Medication |
Child dose |
Adult dose |
|
Oxygen |
Low-flow oxygen is recommended to maintain saturation ≥94% |
Low-flow oxygen is recommended to maintain saturation ≥93%
Providing 28% oxygen is better than 100% oxygen |
|
Salbutamol
Nebulizer solution |
2.5 mg/dose if ≤20 kg body weight 5 mg/dose if >20 kg body weight |
5 mg/dose |
|
MDI (100 mcg/puff) |
4 puffs/ dose ≤20 kg 8 puffs/ dose >20 kg |
8 puffs/dose |
|
Ipratropium bromide
Nebulizer solution MDI (18 mcg/puff) |
0.25 mg/dose 4 puffs/dose |
0.5mg/dose 8 puffs/dose |
|
Prednisone (PO) Prednisone (PO) Methylprednisolone (IV) |
1-2 mg/kg (max.40 mg/day) for 5 days |
50 mg/day for 5 days · It is recommended to be started as soon as possible preferably within 1 hour of presentation in moderate or severe asthma exacerbation · It is usually not necessary to taper the dose unless the duration exceeded 2 weeks |

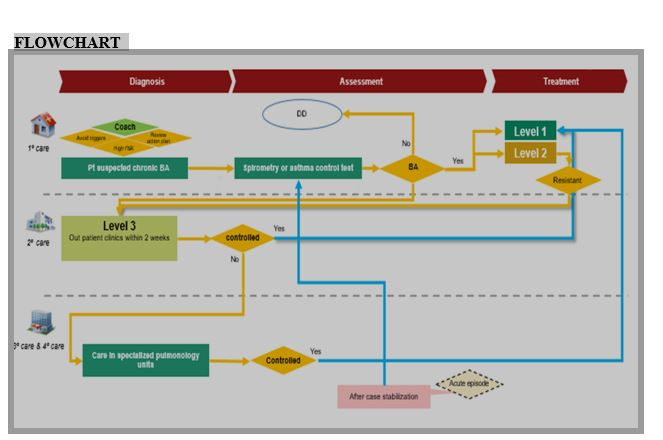
Level 1 (Visit Primary care facilities only)
· BA patient had asthma control test ≥ 20
· PEFR > 80% of predicted personal best
· Spirometry > 70%
Level 2 (Visit Primary care facilities if not controlled within 6 months referred to secondary care)
· Asthma control test: 16- 19
· PEFR: 60 -80 % of predicted personal best
· Spirometry: 60 - 70 %
Level 3 (Visit secondary care within 2 weeks)
· Asthma control test: < 16
· PEFR: < 60 % of predicted personal best
· Spirometry: <60 %
Level 1 (Visit Primary care facilities only)
· Physician assessment of control: 0
· Spirometry: >70%
Level 2 (Visit Primary care facilities if not controlled within 3 months referred to secondary care)
· Physician assessment of control: 1-2
· Spirometry: 60 % - 70%
Level 3 (Visit secondary care within 2 weeks)
· Physician assessment of control: >= 3
· Spirometry: <60 %
{kind=link}