Loading...
Well baby initiative aims to activate and optimize role of PHC in well baby care through a range of services over the first 5 years of his/her life. These clinics will play a major role in supporting parents in raising healthy children by providing vaccination, screening services, psychological support, child safety (including mandatory child car seat check), nutrition education, as well as mentoring growth and development. Each PHC will require one room for check-ups and one treatment room for vaccinations, weighting and measuring the height of babies, and checking their vitals; both rooms should be child friendly. Each clinic will need 1 physician, 2 nurses to efficiently follow the pathway.
Born at term
Weight appropriate for gestational age and not wasted
The history of the pregnancy, labor, delivery and the post delivery period are normal
The vital signs are normal and the infant appears normal on examination
From 0 up to 6 months – normal well-baby, visit primary care facilities only
From 6 months up to 12 months - normal well-baby, visit primary care facilities only
Low APGAR score at the fifth minute
Longer hospital stay after C.S. or complications due to NICU stay
Infants who are born to mothers with a complicated pregnancy, labour or delivery
From 0 up to 6 months – at risk baby, need more assessment, secondary care then primary care for follow-up
From 6 months up to 12 months – controlled well-baby, visit primary care facilities only
Working mother
Poor family
Death of either of the parent or divorce
Bottle feeding (absence of breast feeding)
Mental OR psychiatric disease in either of the parent
Twins
Close spacing (less than 2 years)
Early weaning (before completion of 6 months)
Precious baby (along awaited pregnancy after a period of infertility)
A child not vaccinated
Large family (more than 7 individuals)
Multifactor (if there is more than one risk factor)
From 0 up to 6 months - at risk baby, need more assessment, secondary care then primary care for follow-up
From 6 months up to 12 months - controlled well-baby, visit primary care facilities only
Low birth weight LBW <2.5kg but gestational age is >37 week
Premature child <3 weeks irrespective of weight
Weight equal or below 5% of expected weight for his age
Weight equal or above 95% of expected weight for his age
Failure to thrive (no increase in weight for last three successive visits), even if his health condition is good
If the growth curve (weight) is going down for last 2 successive visits), even if his health condition is good
Those children who do not have 1/2 kg increase per month for the first 3 months of age & 1/4kg increase in weight per month for the 2nd 3months age
Multifactor (if there is more than one risk factor)
From 0 up to 6 months – high risk baby for specialized centers care & tertiary opinion for baby care
From 6 months up to 12 months - at risk baby, need more assessment, secondary care then primary care for follow-up
Birth trauma (anoxia, convulsions)
Handicapped child (mental/ physical)
Bronchial asthma
Congenital heart disease or other congenital defects
Juvenile DM
Diseases of CNS & other like cerebral palsy & mongolism
Red flag of eyes
Red flag of ears
Developmental red flag
Hereditary blood disease like sickle cell disease, thalassemia & others
Hypothyroidism
Renal disorders
Child abuse
Leukemia
Multifactor (if is more than one risk factor)
From 0 up to 6 months - high risk baby for specialized centers care & tertiary opinion for baby care
From 6 months up to 12 months - high risk baby for specialized centers care & tertiary opinion for baby care
From 0 up to 6 months – Acute episode, visit PHC & acute care in specialized centers for patients with comorbidities and urgent cases
From 6 months up to 12 months - Acute episode, visit PHC & acute care in specialized centers for patients with comorbidities and urgent cases
To aid in the early detection of critical congenital heart disease (CCHD) in newborns before discharge from the hospital
To develop strategies for the implementation of safe, effective, and efficient screening
Newborn screening for critical CHDs involves a simple bedside test called pulse oximetry. This test estimates the amount of oxygen in a baby’s blood. Low levels of oxygen in the blood can be a sign of a critical CHD. The test is done using a machine called a pulse oximeter with sensors placed on the baby’s skin. The test is painless an takes only a few minutes
Hypoplastic left heart symdrome
Pulmonary atresia (with intact atrial septum)
Tetralogy of fallot
Total anomalous pulmonary venous return
Transposition of the great arteries
Tricuspid atresia
Truncus arteriosus
Aortic arch atresia or hypoplasia
Interrupted aortic arch
Coarctation of the aorta
Double-outlet right ventricle
Epstein’s anomaly
Pulmonary stenosis/atresia
Atrioventricular septal defect
Ventricular septal defect
Other single ventricle defect (other than hypoplastic left heart syndrome and tricuspid atresia)
*. The secondary defect can be just as serious a primary screening targets but may not be detected as consistently with pulse oximter screening.
*. Passed Screen: an oxygen saturation measure that is ≥95% in the right hand or foot with a ≤3% absolute difference between the right hand or foot is considered a passed screen and screening would end
*. Failed Screen: an oxygen saturation is ≤90% (in the initial screen or in repeat screens), oxygen saturation is <95% in the right hand and foot on three measure, each separated by one hour or >3% absolute difference exists in oxygen saturation between the right hand and foot on 3 measures, each separated by one hour.
*. Any infant who fails the screen should have a diagnostic echocardiogram. The newborns’ pediatrician should be notified immediately and the infant might need to be seen by a cardiologist
Growth assessments
Length, weight & head circumference measurements should be taken with each visit
Well-baby clinic is an excellent place for primary prevention & family education especially on breast feeding & good nutrition
Assessments of the baby’s reflexes and neurological developments
Systemic examinations to detect any childhood diseases from earlier stages
Breastfeeding encouragement
Check total serum bilirubin
Length, weight & head circumference measurements should be taken with each visit
Well-baby clinic is an excellent place for primary prevention & family education especially on breast feeding & good nutrition
Assessments of the baby’s reflexes and neurological developments
Systemic examinations to detect any childhood diseases from earlier stages
Breastfeeding encouragement
Check total serum bilirubin
Head control
Gross motor skills
1st visit to 4th visit (2 month to 9 month) – weight, length, head circumference, temperature
5th visit (12 month) – weight, length, head circumference, temperature, Hb
6th visit (18 month) – weight, height, head circumference, temperature
7th visit (24 month) – weight, height, BMI, head circumference, temperature
1st visit to 3rd visit (2 month to 6 month) – exclusive breast feeding, mixed feeding, only milk formula
1st visit to 10th visit (2 month – 5 years) – assess if patient “with risk” or “no risk”
1st visit (2 month) – DTap, HBV, IPV, Hib, PCV, Rota
2nd visit (4 month) – Dtap, HBV, IPV, Hib, PCV, Rota
3rd visit (6 month) - Dtap, HBV, IPV, Hib, PCV, Rota, OPV, BCG
4th visit (9 month) – Measles, MCV4
5th visit (12 month) – OPV, MMR, PCV, MCV4
6th visit (18 month) – OPV, DTap, Hib, MMR, Varicella, Hepatitis A
7th visit (24 month) – Hepatitis A
8th visit (3 years) - none
9th visit (4 years) - none
10th visit (5 years) – OPV, DTap, MMR, Varicella
*. Overall findings, plan regarding follow-up, medications, health education, referral, next visit data
Clinical examination and basic procedure for early detection of hearing impairment, Congenital heart disease
Laboratory investigations for metabolic disorders
WRHA Primary Health Care Practice Guidelines –Winnipeg Regional Health Authority –May 15, 2018
Child Health Passport – Saudi Arabia – April 1, 2020
1. First Stage:
At birth, a clinical examination and basic procedures are carried out, such as early detection of hearing impairment and congenital heart disease, as well as laboratory tests for some metabolic diseases
2. Second Stage:
It is the one in which the newborn is followed up and is during the postpartum period, when the mother brings her newborn with her for follow-up. It includes two basic visits, the first at the first week of birth and the second visit at the end of the fourth week of the birth, both of which are in the clinic for a healthy child.
3. Third Stage:
It is the one in which the child is followed up from the age of two months until he reaches the age of five years at the will baby clinic, and this phase contains ten timed visits, in which the child's growth and development indicators are measured and clinically examined, in addition to giving him basic vaccinations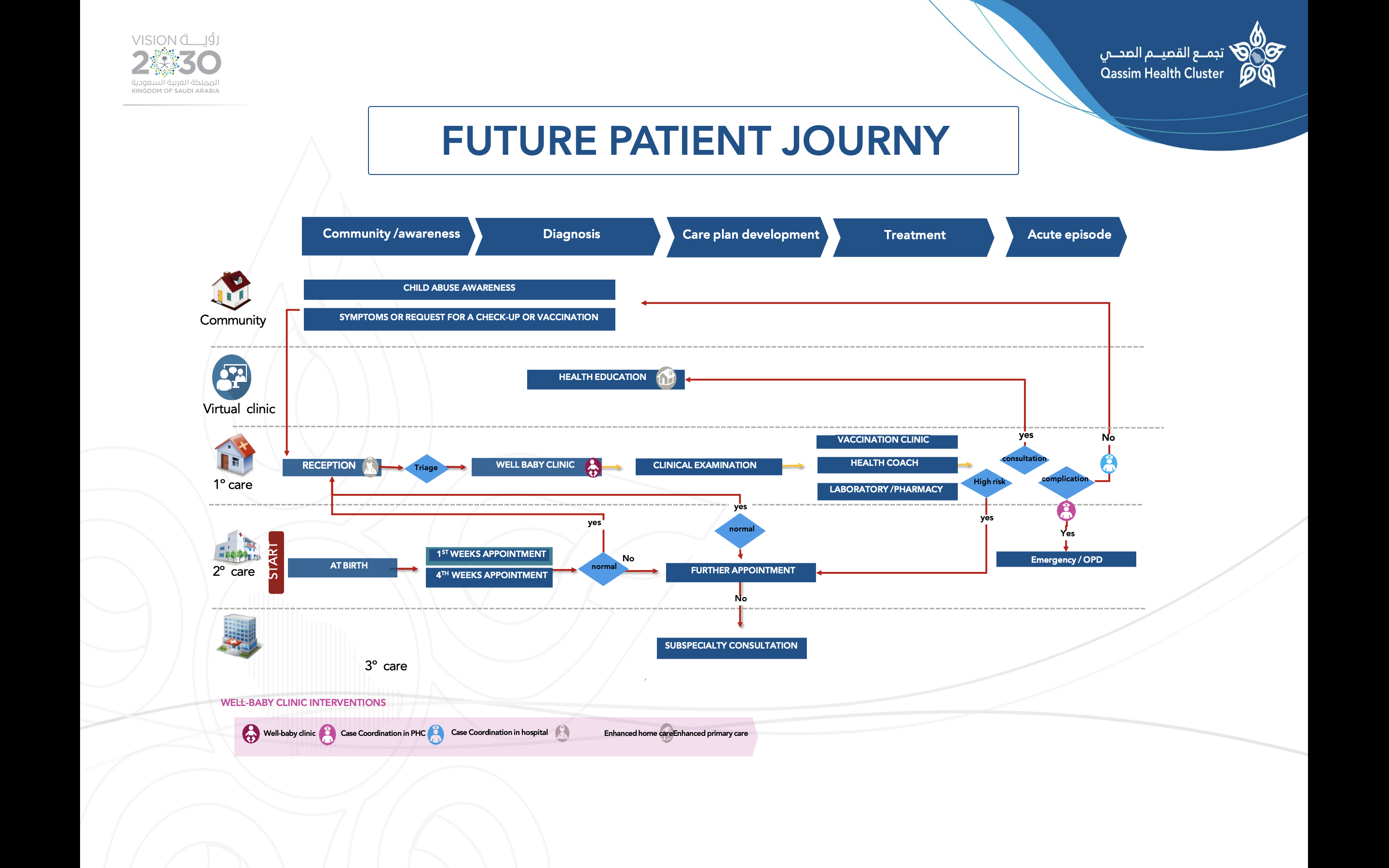{kind=link}