Loading...
Atherosclerotic cardiovascular diseases (ASCVD) is the leading cause of death worldwide and in Saudi Arabia. Dyslipidemia is one of the main risk factors for ischemic heart disease. The overall prevalence in Saudi Arabia ranges from 20% to 40%. The highest prevalence was for triglycerides 44%. Intensive therapeutic interventions plays a major role in reduction of serious cardiovascular outcomes in patients with ASCVD.
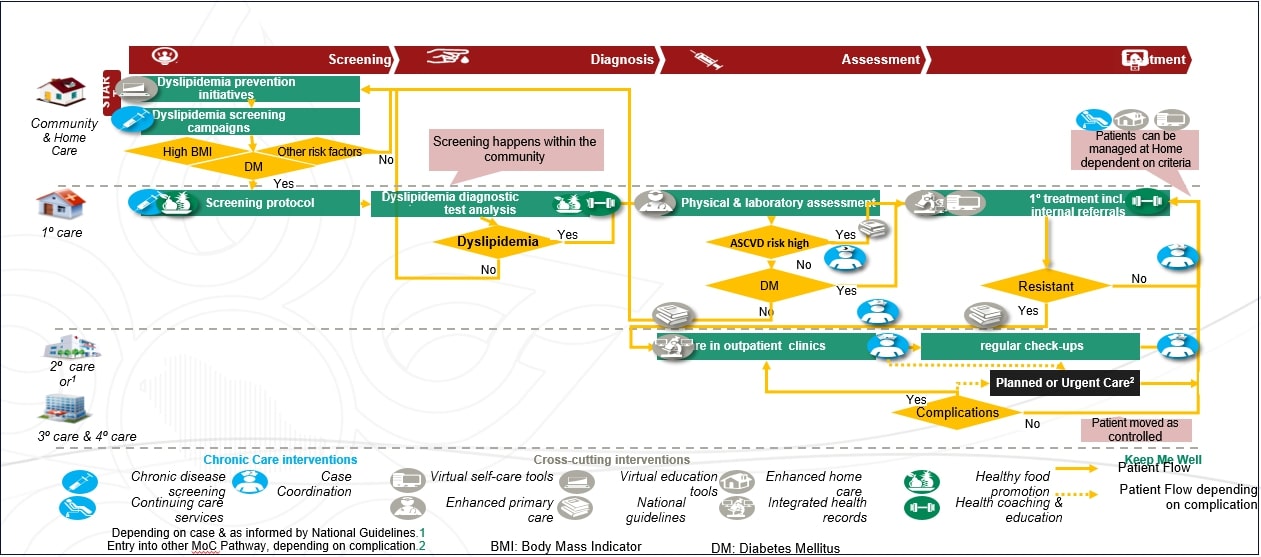
The Ministry of Health has adopted the model of care project that was introduced as part of the new vision of our country (2030) in 2017. The model represents a method for restructuring health care through interactions between health systems and communities.
It focuses on the patient's journey through health system and help to provide an organized, coordinated, and patient centered healthcare services. The outcomes of this model will be reflected on cost reduction, decrease in morbidity and mortality from chronic diseases as well as increase the satisfaction of patients and their caregiver.
Appendix 3: Secondary Prevention in Patients with Clinical ASCVD
The following patients will be referred to the tertiary Hospitals:
Re-evaluate ASCVD risk after lifestyle and secondary factors are addressed.
Statin-Associated Side Effects.
Therapeutic lifestyle changes:
Increase exercise .
Screening and Referral Guidelines:
Referral Guidelines
Standard lipid panel:
Liver transaminase (AST, ALT) levels:
{kind=link}